All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.

The Multiple Myeloma Hub is an independent medical education platform, sponsored by Bristol Myers Squibb, GSK, Legend Biotech, Pfizer, and Roche. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View multiple myeloma content recommended for you
Outcomes with novel CELMoD agents for MM
Do you know... In the phase I/II CC-92480-MM-002 study, durable PFS exceeding 12 months was observed with MeziVd/MeziKd in patients with how many prior lines of therapy (LOT)?
The treatment landscape for multiple myeloma is continually evolving with the introduction of novel agents. These options have led to improved outcomes and extended survival, yet most patients will eventually experience a relapse.1 Patients who relapse often develop resistance to prior therapies. Lenalidomide, an immunomodulatory agent (IMiD), is used widely both in frontline regimens and as maintenance therapy for patients with newly diagnosed multiple myeloma (NDMM), and as a result, a proportion of patients are refractory to lenalidomide by the time of first relapse.1 This has led to an unmet need for therapies that retain activity in patients with multidrug-refractory disease, particularly in those with prior IMiD exposure or refractoriness.1
Cereblon E3 ligase-modulating drugs (CELMoDs) are an emerging class designed to overcome some of the limitations of earlier IMiDs. CELMoDs act to engage the receptor cereblon (CRBN) of the cullin 4a-cereblon cullin-RING ligase (CRL4CRBN) E3 ubiquitin ligase complex, promoting ubiquitination and proteasomal degradation of key transcription factors such as Ikaros and Aiolos.1 CELMoDs are distinguished from IMiDs by their enhanced binding to cereblon, more rapid or deeper substrate degradation, and often more potent immune-stimulatory effects.1 These characteristics may allow CELMoDs to remain effective even in patients who are refractory to lenalidomide and pomalidomide.1
There are currently two oral CELMoDs in clinical development for the treatment of both NDMM and relapsed/refractory multiple myeloma (RRMM): mezigdomide and iberdomide.1 An overview of ongoing clinical trials of mezigdomide and iberdomide has been published previously by the Multiple Myeloma Hub.
Mezigdomide
Mezigdomide has demonstrated antimyeloma activity, including in patients with heavily pretreated and lenalidomide-refractory disease. Mezigdomide has shown efficacy both as monotherapy and in combination regimens, with ongoing clinical studies further evaluating its role in combination in the relapsed/refractory setting.1
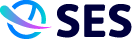
During the 22nd International Myeloma Society (IMS) Annual Meeting, September 17–20, 2025, Toronto, CA, the latest data were presented on mezigdomide in combination with dexamethasone and either bortezomib or carfilzomib (MeziVd or MeziKd) for patients with RRMM.2 This analysis, from the phase I/II CC-92480-MM-002 trial, evaluated efficacy by prior lines of therapy to help define mezigdomide’s potential place in the treatment paradigm and its benefits for heavily pretreated patients – an area of significant unmet need.2
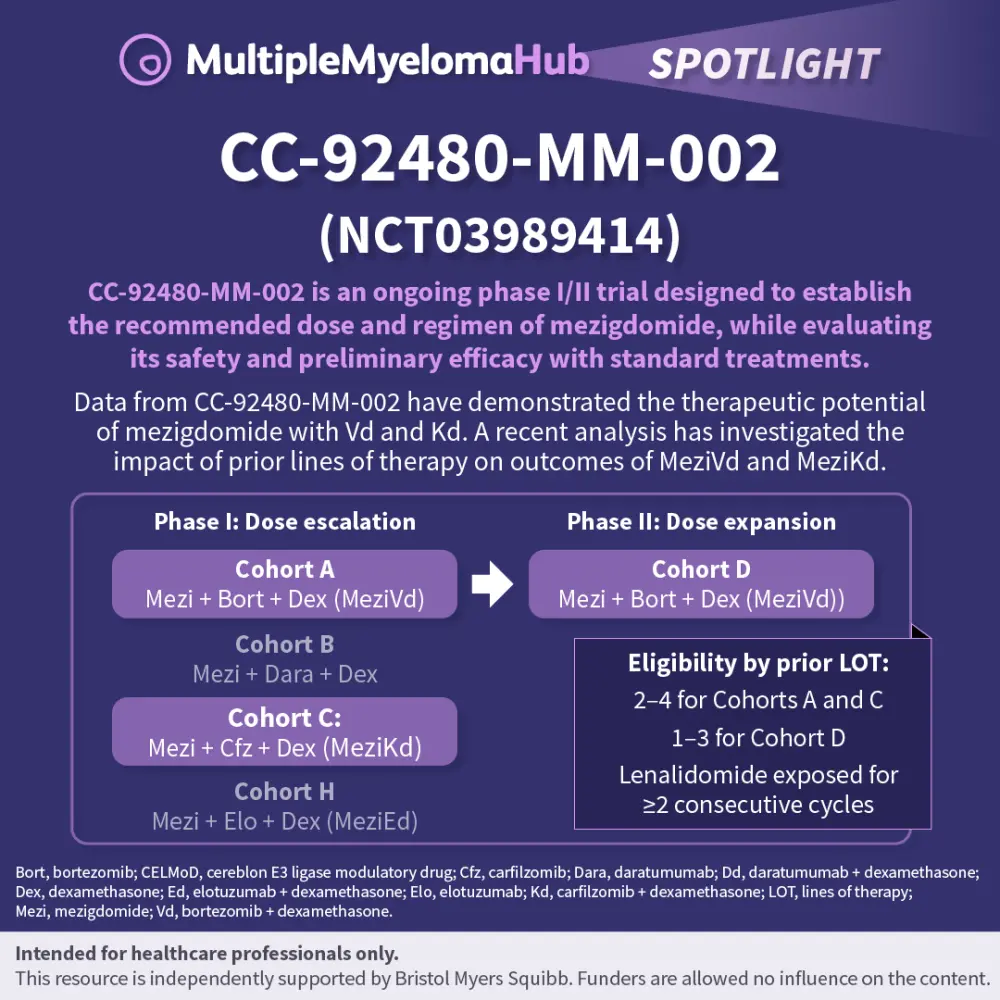
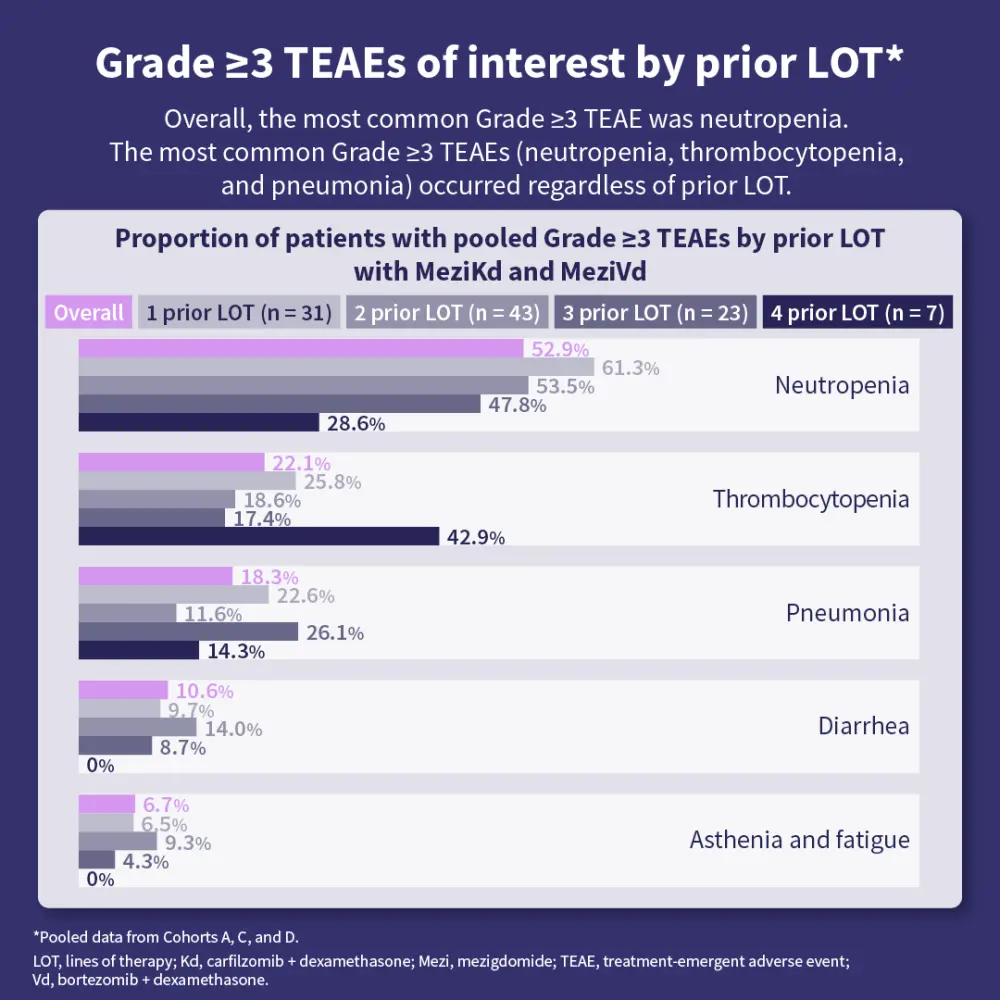
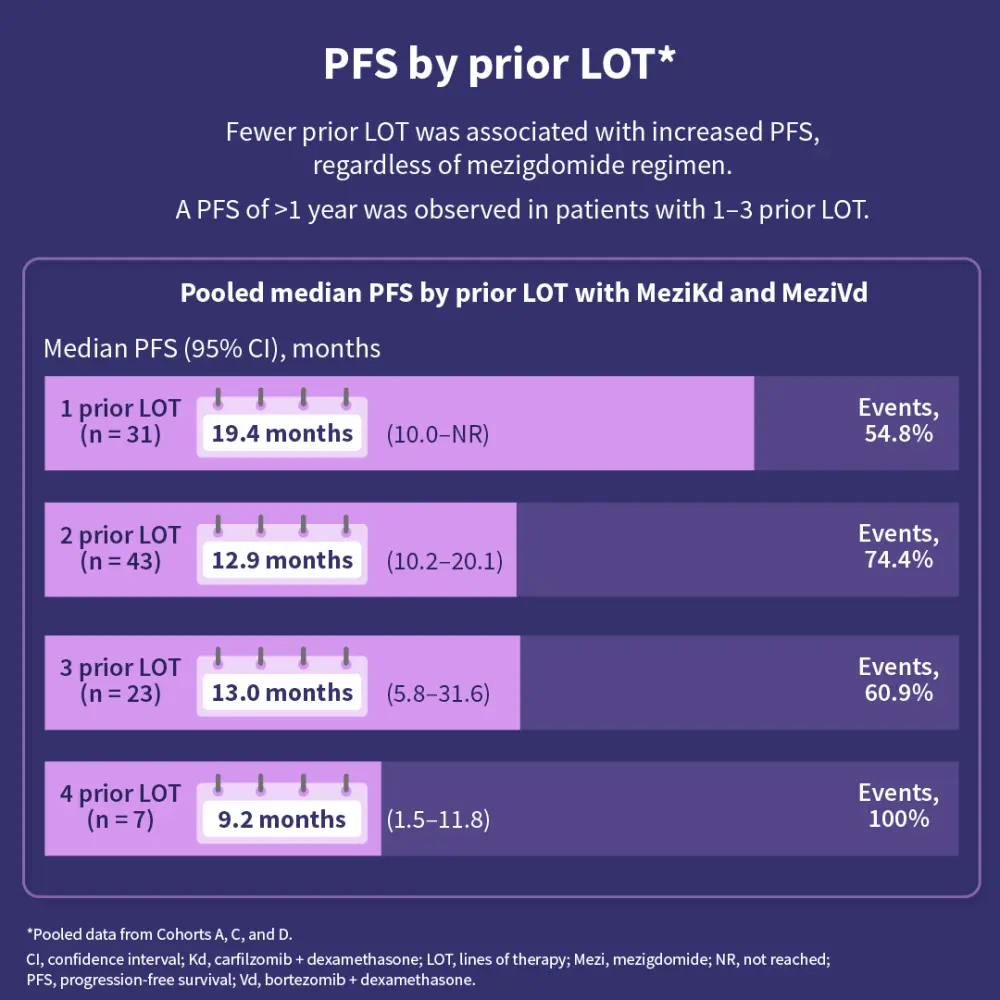
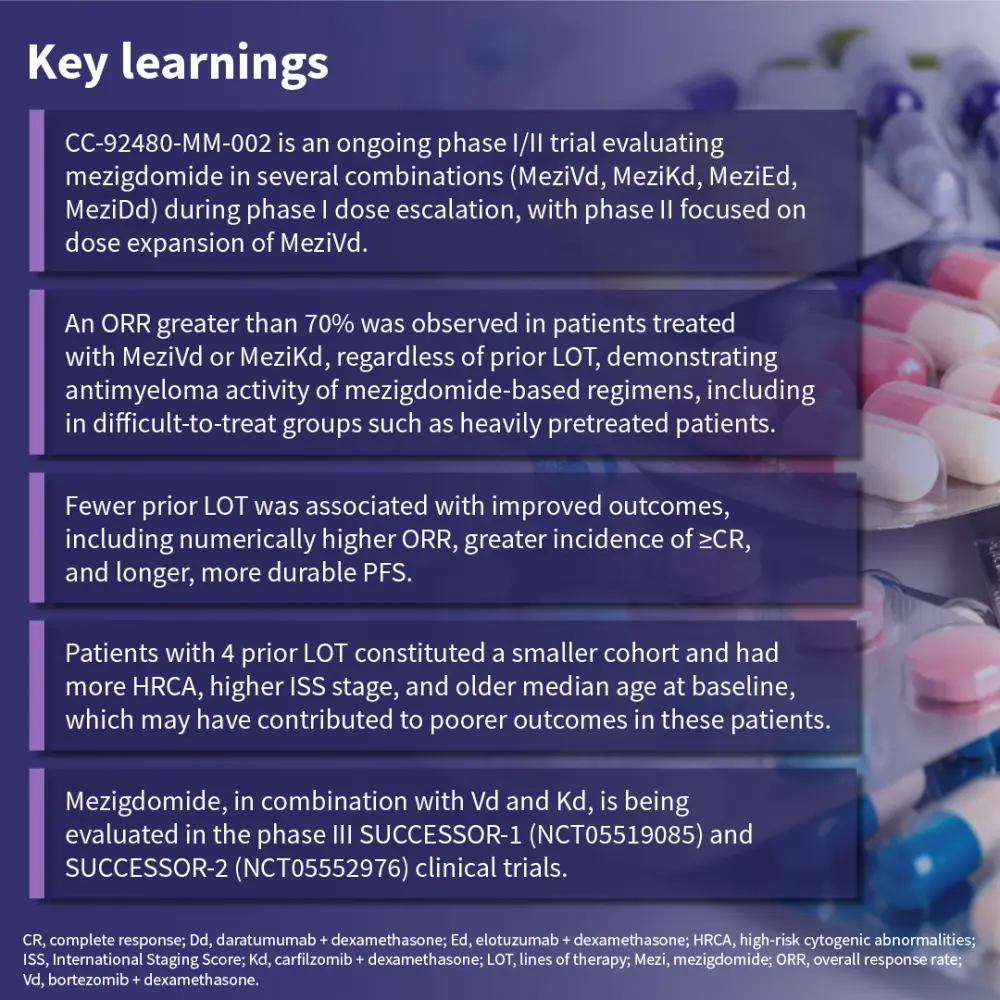

Mezigdomide-based combinations demonstrated antimyeloma activity across patient groups, with outcomes generally favoring those with ≤3 prior lines of therapy.2 Ongoing phase III trials, SUCCESSOR-1 and SUCCESSOR-2, aim to further define the role of mezigdomide-based regimens and their potential to improve outcomes for patients with RRMM.1,2
Iberdomide
Iberdomide has shown efficacy in early studies as both a monotherapy and in combination with established antimyeloma agents.1
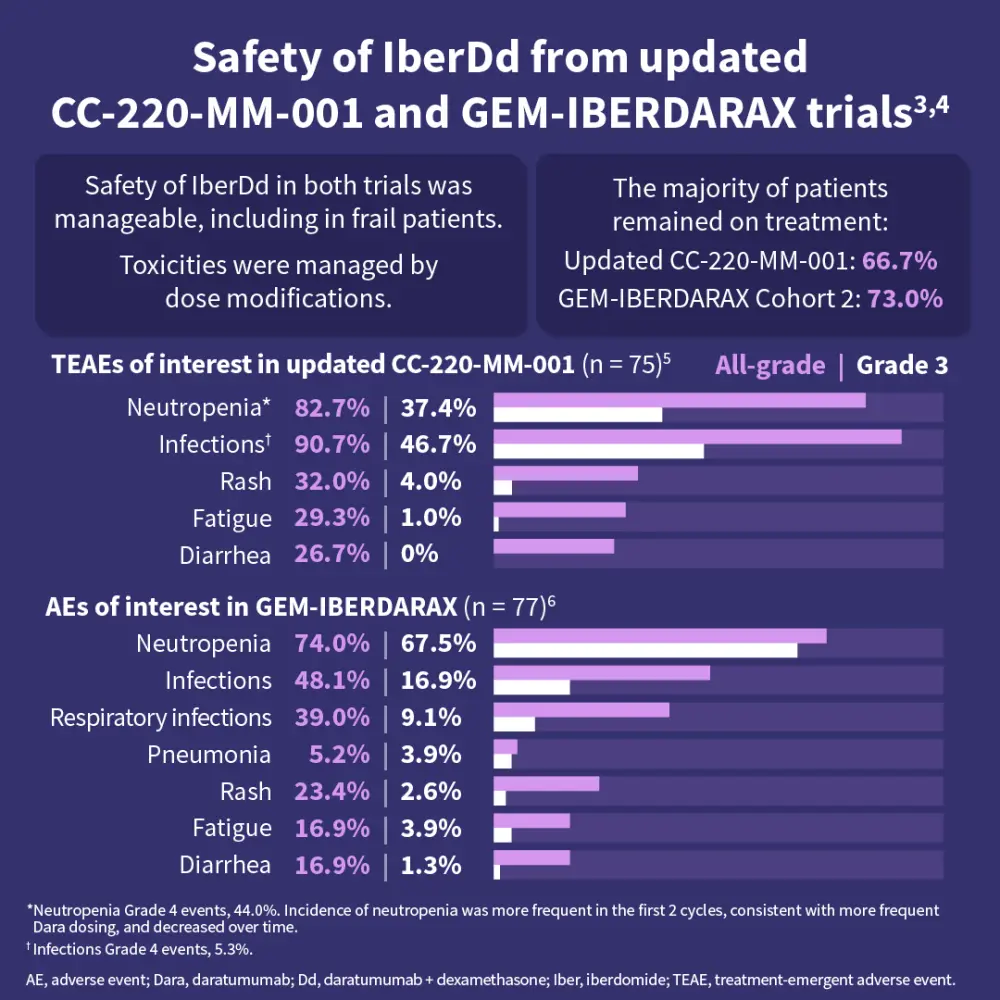
During the 22nd IMS Annual Meeting, the latest data were presented on iberdomide in combination with daratumumab + dexamethasone (IberDd) for the treatment of transplant ineligible/deferred NDMM from the phase I/II CC-220-MM-001 and the phase II GEM-IBERDARAX trials.3,4
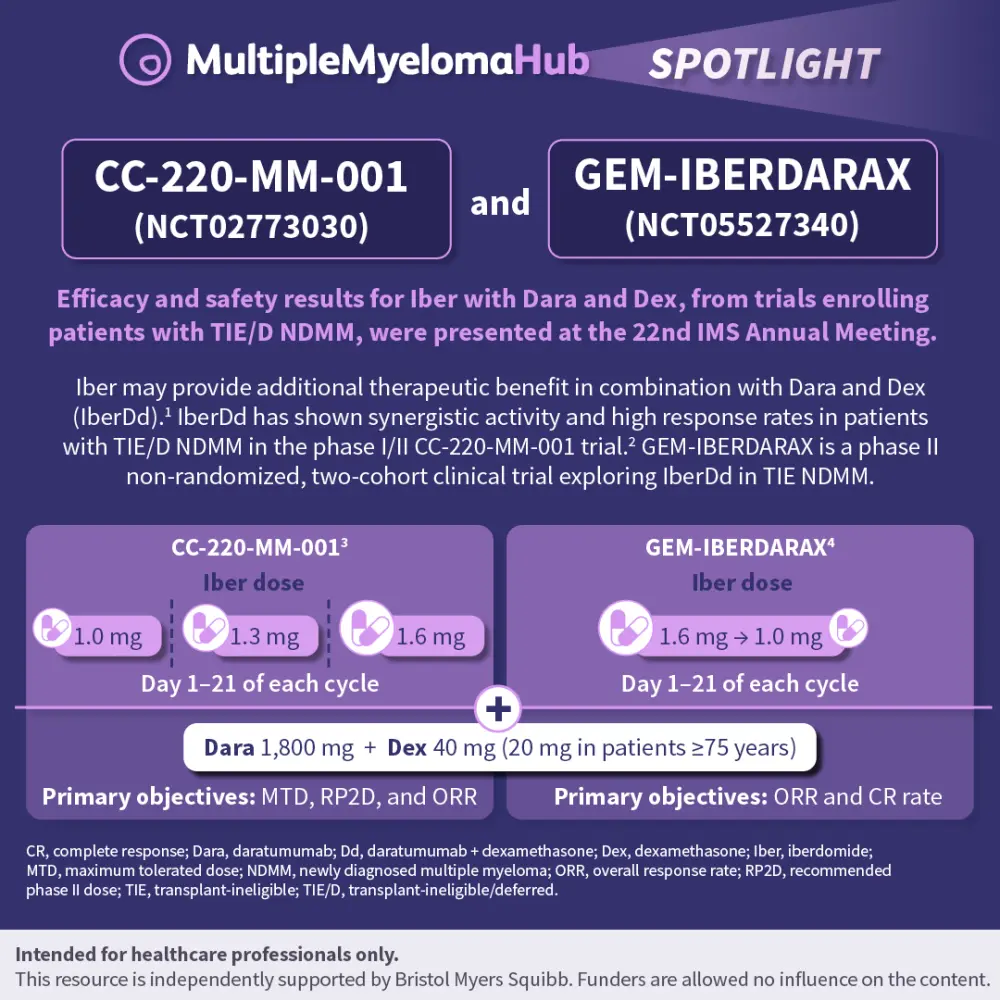
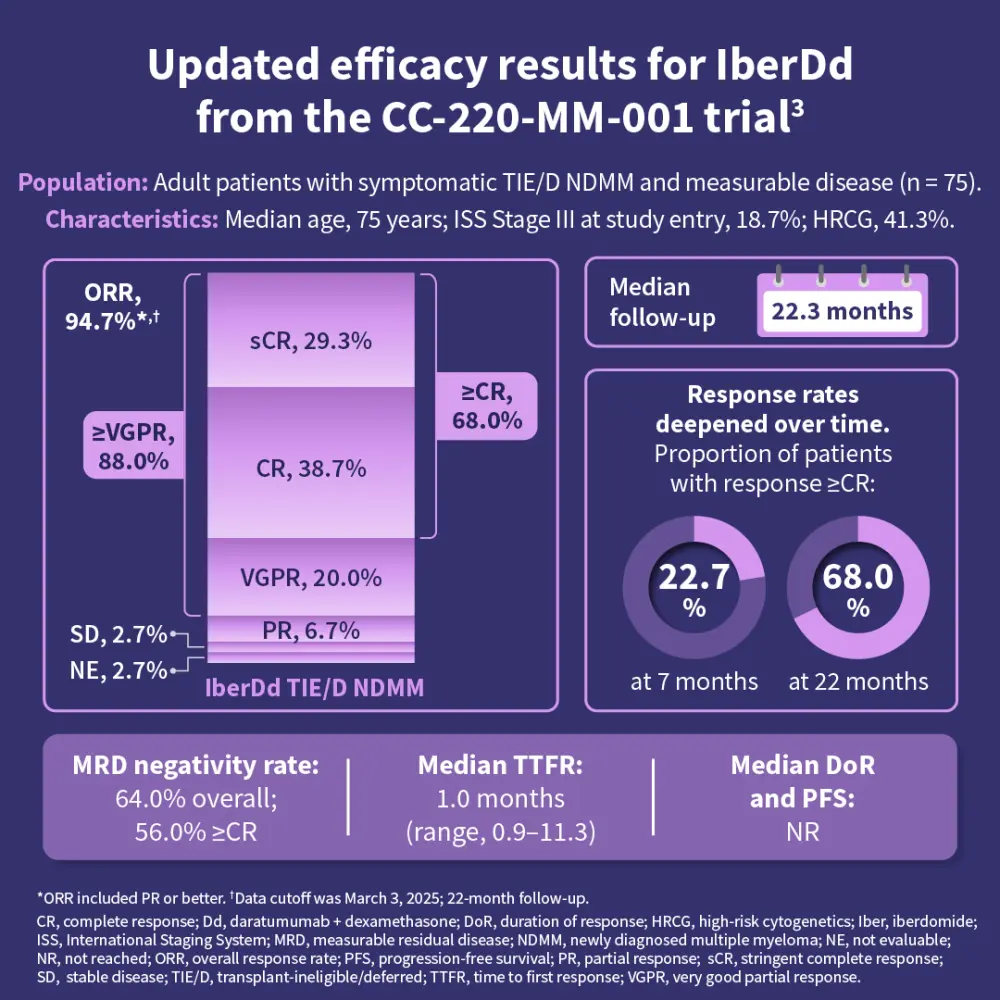
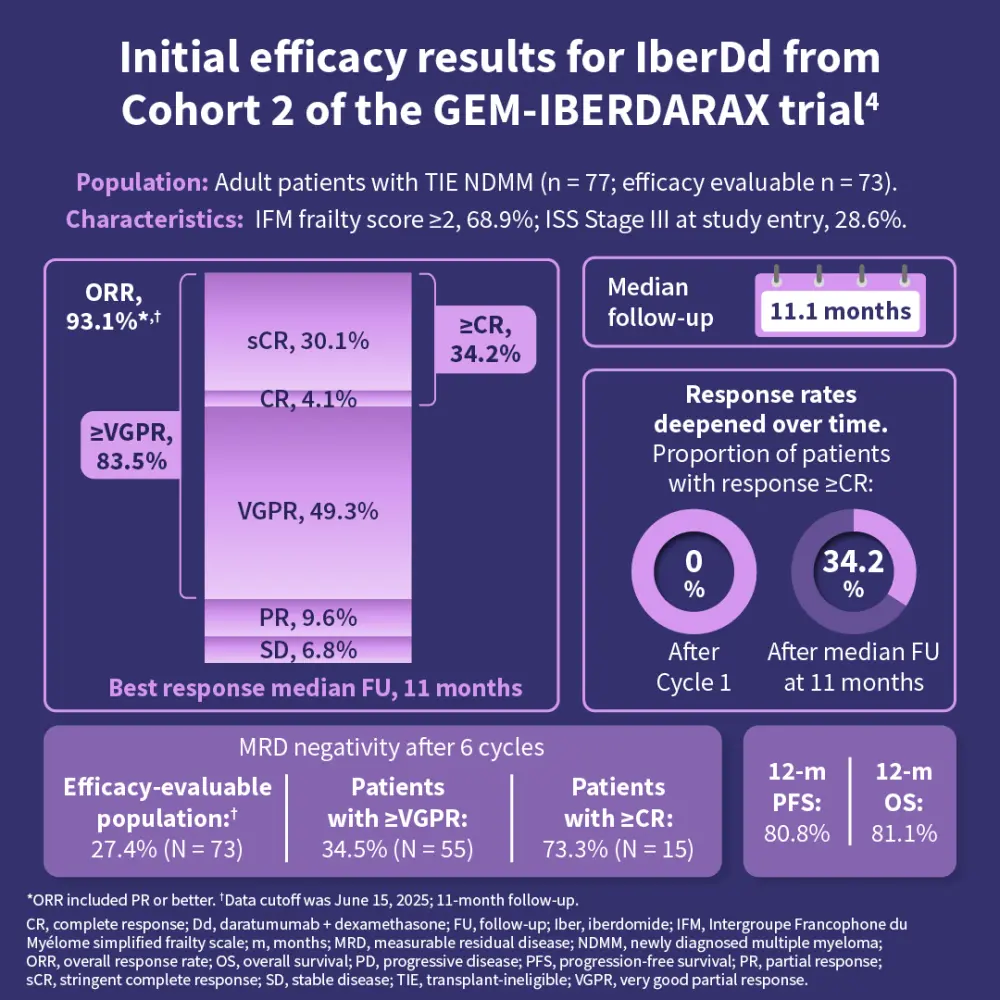
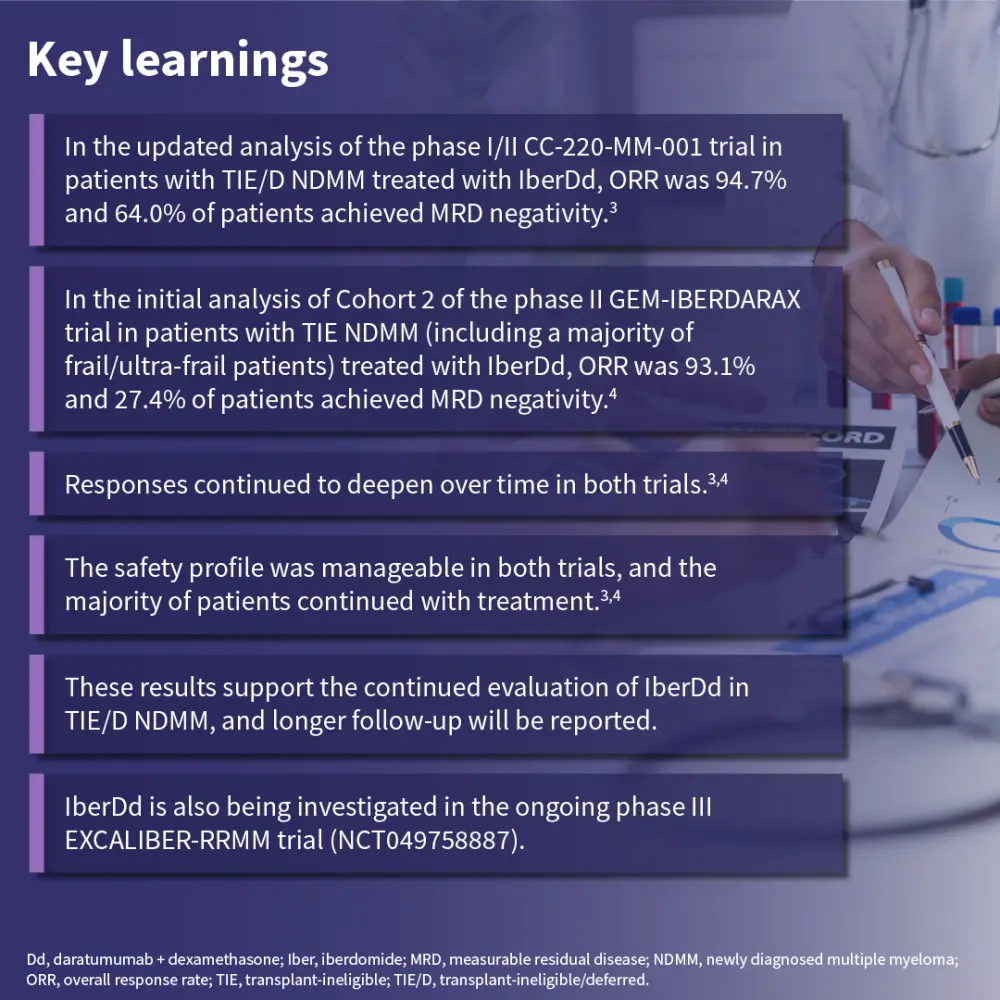
The IberDd combination has been identified as a promising therapeutic option for further evaluation in phase III studies, in both NDMM and RRMM.1,3,4
Key takeaways
The emergence of CELMoDs represents a promising advancement in addressing the unmet need for patients with RRMM, particularly those with prior IMiD exposure or lenalidomide-refractory disease.1 Early clinical data with mezigdomide and iberdomide demonstrate antimyeloma activity, both as monotherapy and in combination regimens.1 Results from ongoing phase III trials will help refine their place in the treatment landscape for MM and their potential to expand effective therapeutic options for patients with newly diagnosed and relapsed/refractory disease.1
This educational resource is independently supported by Bristol Myers Squibb. All content was developed by SES in collaboration with an expert steering committee. Funders were allowed no influence on the content of this resource.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
Your opinion matters
On average, how many patients with MGUS/smoldering MM do you see in a month?